For many years I was a prisoner of a futile struggle against my own suffering. I struggled so long that I naturally developed a burning passion for psychotherapy effectiveness and for quick and effective approaches. This is how I came to evidence-based and scientifically-validated approaches, such as Acceptance and Commitment Therapy (ACT pronounced as “act”) that I practice today. Thus, being effective for my clients and working tirelessly to improve my professional skills are two of my central values as a psychologist.
Psychotherapy Effectiveness: A Shameful Secret
One of psychotherapy’s shameful secrets is that, on the whole, therapist effectiveness is not very high. Even though research shows that for one person in two, therapy will be useful and effective, still, one person in two to one person in three will see no benefit from going to therapy. Before rejecting therapy as useless, remember that, without treatment, fewer than one person in three gets better. That said, it’s clear that our profession can do better, much better.
Psychotherapy Effectiveness: Where We Are
In statistics, we measure effect sizes, that is how much people get better (or worse) following treatment. To get a sense of effectiveness across many studies, researchers conduct meta-analyses. These group thousands of individual outcomes to get to the big picture view. Thus, meta-analyses have shown that psychotherapy’s effect sizes across problems and approaches vary between .5 and .9. An effect size of .5 is considered clinically significant, meaning that people experience getting better with respect to what brought them into therapy (Hunsley, Elliott, & Therien, 2013 for a Canadian Report on psychotherapy effectiveness).
Psychotherapy Effectiveness in Real Life
Studies of therapist effectiveness outside the confines of tightly controlled scientific studies, i.e. the kinds of therapists you’re most likely to hire, suggest a similar effectiveness (.8 on average). But, the bad news is that experienced therapists don’t seem more effective than graduate students (Minami et al., 2009). Goldberg and colleagues (2016) even reported that therapist effectiveness could decrease with time and experience!
Bruce Wampold, a leading researcher in the field thus offers a disheartening conclusion: “Therapists do not get better with time or experience. That is, over the course of their professional careers, on average, it appears that therapists do not improve, if by improvement we mean ‘achieve better outcomes’.” (Wampold & Imel, 2017).
ACORN
What to do to increase psychotherapy effectiveness? Inspired by my friend and Australian colleague Julian McNally the Contextual Psychology Center joined the ACORN collaboration. This network brings together over 15,000 clinicians from several countries who practice a broad range of psychotherapy approaches. ACORN members have made the choice to measure their effectiveness and invite their clients to fill in a brief questionnaire at the outset of each session.
Because the questions asked have been selected among hundreds as the ones most likely to capture common problems and measure psychotherapy effectiveness, ACORN is a valuable tool. This way, ACORN has collected data which demonstrates that using their questionnaires and using the data they generate to guide one’s practice is associated with improved effectiveness. (Brown & Simon, ACORN report). This is why I now use the ACORN questionnaires with all my clients.
Catastrophe
For many clinicians, measuring our efficacy can make us feel insecure and appear scary. Yet, it is essential if serving our clients well is important to us. So I chose to face my fears and fed my clients’ data into the ACORN database. After about 10 clients, the system returned that my overall effectiveness was below .3. Pitiful.
I went to discuss the result with a colleague. “Look at this,” I said disheartened. “I always knew and said I was a better trainer than clinician.” Without missing a beat she replied: “I think you’re even worse at data entry.” She was right. I went to check and I had made a complete mess of entering my clients’ data. Now I get them to feed in their scores straight into ACORN, so as to protect us all from my limitations.
My Commitment
At the CPI, I am committed to improve my effectiveness and to go get support and engage in deliberate practice exercises that, according to research, can help therapist sharpen their skills (Chow et coll. 2015). To support our practitioners, CPI maintains a peer supervision group where we can share our improvement goals and objectives and engage in deliberate practice so as to be even more effective for you.
This is why I commit to regularly update this blog with my latest ACORN scores relative to those of the whole international ACORN community of mental health professionals.
My Current Psychotherapy Effectiveness
Below are my effectiveness scores.
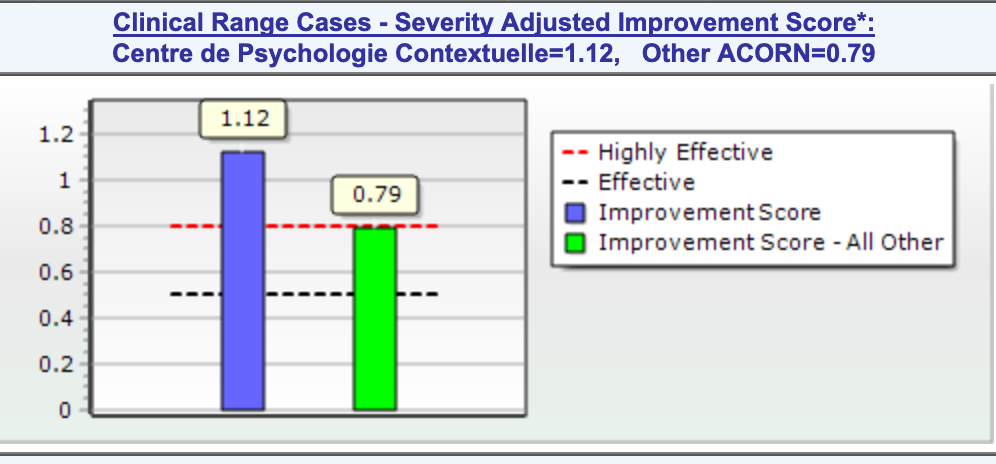
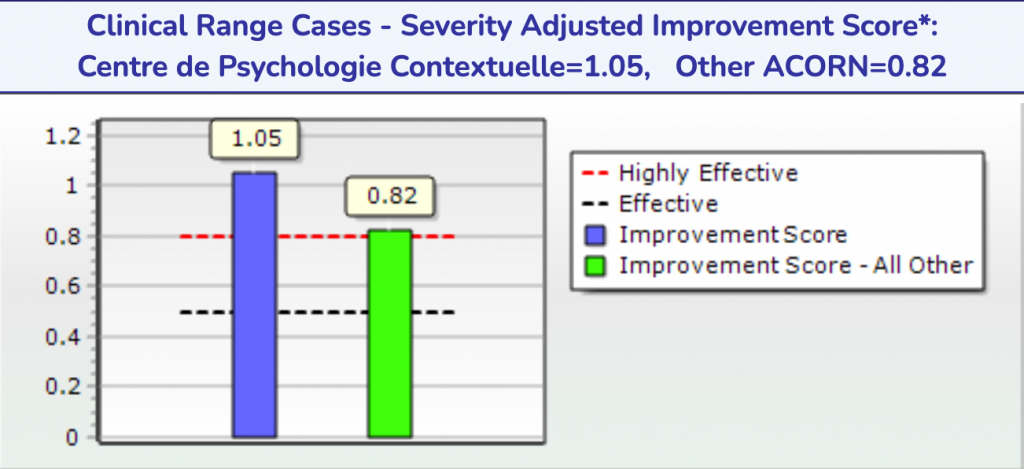
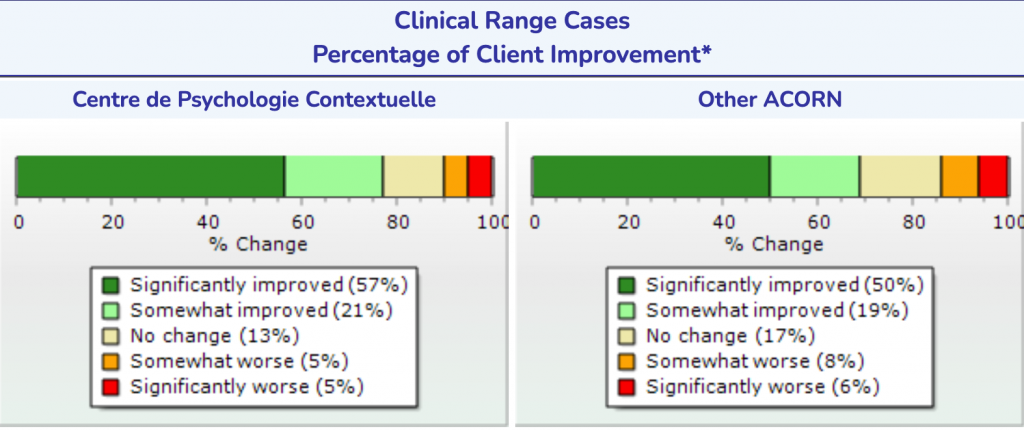
The right-hand side of the diagrams diagram presents the scores of all the mental health professionals members of the ACORN network, the left-hand side my own. For ACORN collaboration members, the average effect size is .81. 69% of ACORN members’ clients get better, 17 % experience no change and 14% get worse.
My own scores to date are given below. My latest effectiveness to June 8th, 2021 : average effect size of 1.04. Of my clients that meet the clinical threshold, 78% report an improvement, of which 57% a significant improvement, and 21% a mild improvement. 13% report no change, 5% a mild deterioration and 5% a significant deterioration. Regarding the latter, note that some treatments are still ongoing.
At the CPI, being effective is not an empty promise, it’s a value we are putting in action!
Mon efficacité clinique vs la moyenne ACORN au 8 juin 2021
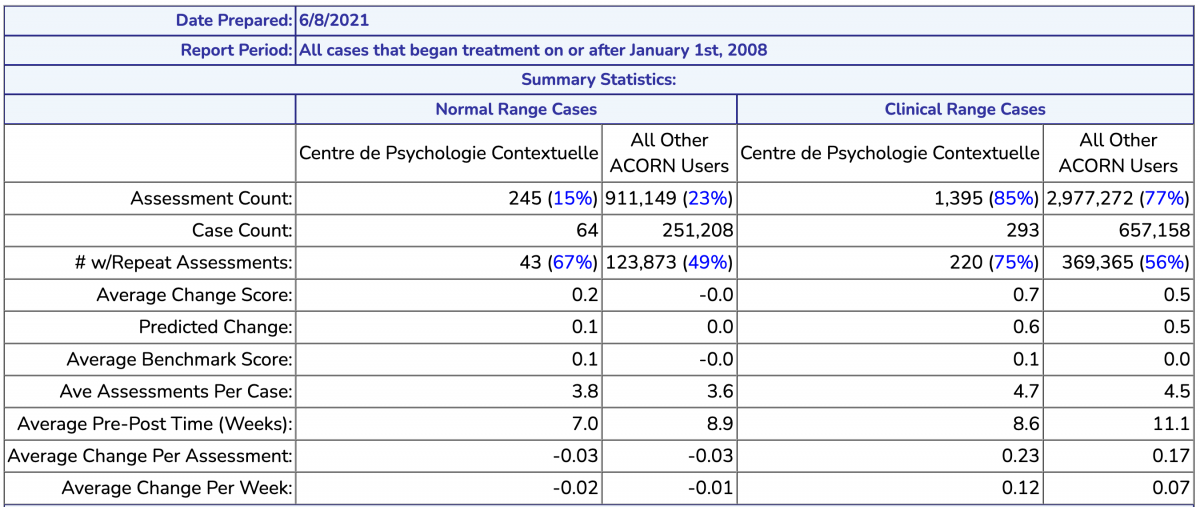
Comparative details of my results vs the ACORN average. My therapies with clinical clients last about 8.6 weeks vs. 11.1 weeks for the ACORN average.
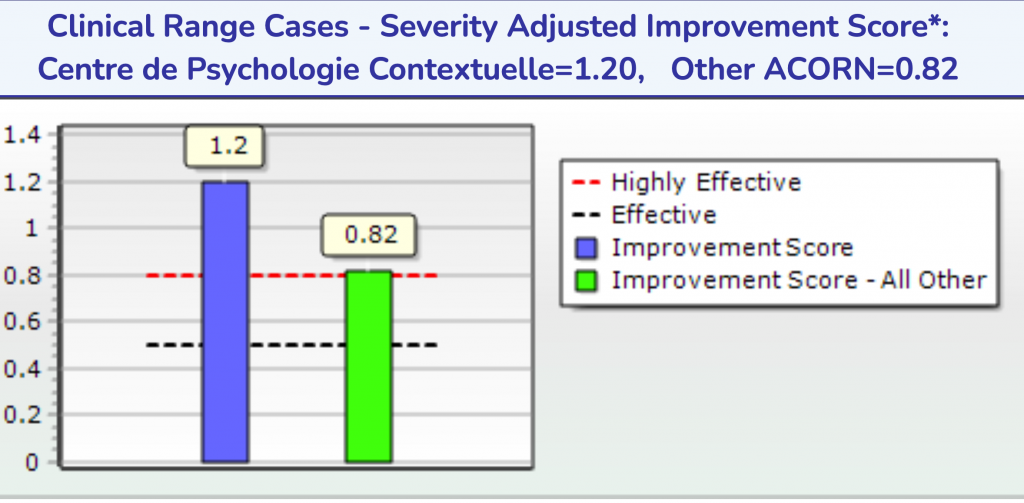
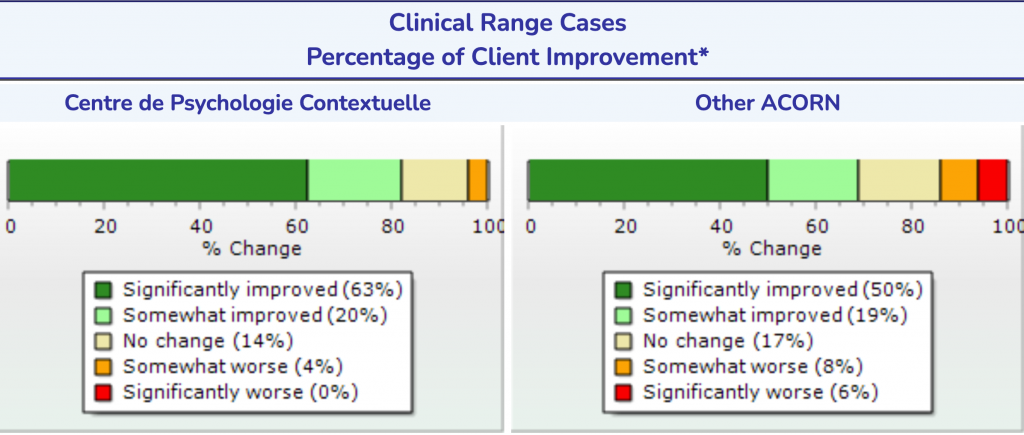
My score for the last 6 months to June 8th, 2021. Effect size 1.2. 83% improved (63% significantly, 20% somewhat. 14% no change, 4% somewhat worse and 0% significantly worse.
Brown, G. S., Simon, A., Cameron, J., & Minami, T. (2015). A collaborative outcome resource network (ACORN): Tools for increasing the value of psychotherapy. Psychotherapy, 52, 412–421. doi: 10.1037/pst0000033
Brown, G. S., Simon, A., & Minami, T. (2015). Are you any good…as a therapist? http://societyforpsychotherapy.org/are-you-any-good-as-a-therapist/
Chow, D. L., Miller, S. D., Seidel, J. A., Kane, R. T., Thornton, J. A., & Andrews, W. P. (2015). The role of deliberate practice in the development of highly effective psychotherapists.
Goldberg, S.B. , Rousmaniere, T. , Miller, S.D. , Whipple, J. 4 , Nielsen, S.L. , Hoyt, W.T. , & Wampold, B.E. (2016a). Do Psychotherapists Improve With Time and Experience? A Longitudinal Analysis of Outcomes in a Clinical Setting. Journal of Counseling Psychology, 63 (1), 1-11.
Hunsley, j., Elliott, K., & Therien, Z (2013) The Efficacy and Effectiveness of Psychological Treatments. A report for the Canadian Psychological Association chiffreshttps://www.cpa.ca/docs/File/Practice/TheEfficacyAndEffectivenessOfPsychologicalTreatments_web.pdf
McNally, J. (2017) What Makes Act of Living Therapists 10% better (Blog) http://www.actofliving.com.au/resources/blog/item/13-ten-percent-better-therapy
Minami, T., Davies, D. R., Tierney, S. C., Bettmann, J. E., McAward, S. M., Averill, L. A., Huebner, L. A., Weitzman, L. M., Benbrook, A. R., Serlin, R. C., & Wampold, B. E. (2009). Preliminary evidence on the effectiveness of psychological treatments delivered at a university counseling center. Journal of Counseling Psychology, 56, 309-320. doi:10.1037/a0015398 14
Wampold BE & Imel Z (2017) http://societyforpsychotherapy.org/what-do-we-know-aboutpsychotherapy-and-what-is-there-left-to-debate/